

Makair: How to solve a crisis by creating a low-cost ventilator in community?
Makair: How to solve a crisis by creating a low-cost ventilator in community?


👋 Hey, it’s Jaime. Welcome to my weekly newsletter, where I share how thriving open-source projects grow their communities.
Subscribe to get access to these posts and all future posts.
In this week’s newsletter, I’m going to show you how Makair developed in a month a ventilator that was 10 times cheaper than the existing offers by breaking down how they rallied a community around a super ambitious mission.
This way, you’ll understand how to create your big ideas even if you don’t have the necessary skills or resources, whether a crisis strikes or not.
We’ll cover:
Understanding the problem and prioritizing what we’ll focus on
How to form an Ecosystem: Setting up an ambitious mission and starting small
Finding better solutions: Starting from first principles while ensuring safety
The importance of embracing existing institutions
Being vulnerable to invite others (but not everyone) to fill in the gaps
How to produce at scale
TL;DR
Read-time: 13 minutes
When a crisis hits, most of us want to do something about it, but they are often so complex that we miss the resources, skills, time and money to solve them.
Crisis create all sorts of shortages. The Covid pandemic left us with a ventilator (and toilet paper) supply shortage. During a war like the one in Ukraine, electricity centrals become targets and leave the country without energy. Or during earthquakes that affect nuclear plants, people need to track radiation without enough Geiger counters.
The good news is that when a problem is shared by many people, crisis or not, we often forget that the most important role is held by the people willing to lead to connect those who can build the solution.
So in today’s issue, I’ll show you how Makair gathered a community of people ready to pool their skills, money and resources to achieve some incredible achievements:
It took them only one month to go from idea to certification application, where hospitals could start testing the first prototypes., which is an absolute feat in medical technology.
Their ventilator was ten to four-hundred times cheaper than what was already available on the market. Usually a ventilator costs between 10,000 to 45,000€ for the most expensive models, and Makair achieved an unbeatable production cost around 1,000€ in 2020, and expects to go as low as 100€ per ventilator in 2024. The more expensive ventilators have a few more settings, but Makair’s alternatives are a lot more affordable and scalable to produce in times of crisis.
Let’s dive in.
Step 1: Understanding the problem
To start, you need to understand what you’re up against, and prioritise where you can contribute.
Makair and theMakers for Life collective was initially launched by Quentin Adam, the director at Clever Cloud, a software company for IT automation. He was later joined by friends at Crips and Pierre-Antoine Gourraud, who heads the “data clinic” at Nantes Hospital.
On March 16 Emmanuel Macron’s “We are at war” speech motivated Quentin Adam, and made him realise that something was going on.
As an entrepreneur, he was already busy with work that was not related to Covid-19. But his girlfriend works in medicine. So he asked her to explain the issues with Covid.
She explained that the severe acute respiratory syndrome can worsen to the point where people need to be put on ventilators, and there were three main problems with that:
The health system faced the risk of being totally saturated, as there were not enough ventilators available.
The existing ventilator offer was unaffordable for many regions.
Given how ventilators are built, it’s very difficult to scale up production in a short period of time because the components were expensive, because they haven’t been designed to be produced in quantities of 200 a year, and because they depended on parts that were not available anymore.
One of the leading manufacturers of respiratory aids in Europe is Hamilton Medical. During the March 2020 lockdown in Europe, this Swiss company increased its production by 50% to meet hospitals’ demand of 1,200 to 1,500 units within a few weeks (the same number of devices usually produced within a year). The company was unable to meet the demand, not only because of limited production capacity, but because it was unable to obtain essential components, as many countries had banned the export of certain medical equipment to prevent domestic shortages.
From these observations, the question was: “Can we build in record time a machine that will allow us to deal with the pandemic?”
To find the constraints they needed to overcome, they had to mirror their problems into solutions and create ventilators that were:
Comparable with expensive hospital reanimation ventilators
Cheap
Made with tools and parts easily available locally, everywhere in the world
Easy to manufacture at scale
He researched a few videos online on the topic and thought it was possible.
Step 2: Forming an Ecosystem by setting up an ambitious mission and starting small
How do you gather a lot of support quickly, from both makers and multiple industries?
Once you understand the contours of the problem, make a list of those who need the solution you want to create and can contribute with the skills, money, tools or facilities you’re lacking.
To inspire them and rally their support when reaching out to them, think of an ambitious goal that’s aligned with their urgent need.
For example, to gauge the interest of potential contributors from other entrepreneurs and medical professionals, Quentin Adam called his colleague Emmanuel Feller, who works with him, as well as fellow entrepreneurs Baptiste Jamin and Valérian Saliou from Crisp, and Pierre-Antoine Gourraud at Nantes’ Hospital, to see if they were interested in tackling the design of a ventilator.
Pierre-Antoine Gourraud is a professor and hospital practitioner at the CHU who co-heads the “data clinic”. He became one of the co-founders of the Makair project, was the link to the hospital and got some of his colleagues involved too.
To rally these first contributors, Quentin Adam invited them to join an ambitious mission: To quickly produce an artificial respirator to overcome the shortage that was about to collapse the healthcare system. This ventilator would have to be open source so it could be available worldwide.

And to understand what was needed, they sought out anesthetists who would use the device to understand their needs. As they interviewed them, they could explain what was required for these devices. Most anesthetists don’t know how a ventilator is built; what counts for them is its operation and parameters. But a precious few of them were able to provide them with the information needed to establish a list of specifications and start tinkering.
So these first contributors became crucial to providing the necessary credibility as well as defining the initial technical specifications for the ventilator. This would create the conditions to invite contributors for the next phase.
Step 3: Start from first principles, don’t copy what’s already been done, and make sure it’s safe to use!
Next, you need to avoid copying what others have done before.
Makair understood that they couldn’t copy what other ventilator manufacturers did because they would end up competing on their components and supply chains and because it could also infringe on their patents.
When we encounter difficult problems, it can be tempting to reason by analogy and rely on what others believe is true. Instead, the Makair team worked on applying first principles to break down the problem into its most fundamental elements and come up with the simplest components they needed to build their ventilator.
Makair was started by software engineers with only a basic knowledge of global engineering or physics.
So instead of starting with a hardware machine running on a bit of software, they started off by designing a software machine, then gradually added what they needed from cheap off-the-shelf parts available.
But they also needed to think ahead.
After prototyping, they needed to understand how they were going to mass produce their devices:
The supply part was crucial if we wanted to industrialise, for example importing parts from China, Ultem medical plastic, etc. Sandra and Morgane, who had experience working with industrial suppliers, nagged them for information about available quantities, etc.
Available supply guided our choices in development. It’s important to understand that engineering was only one aspect of the problem. Knowing the quantity of available stock was crucial, we couldn’t just ask the factory to restart production if we were in short supply. — Quentin Adam
And there was another final hurdle they would need to go through: respecting regulations and certifying their devices for medical use.
They soon realised that their initial vision of “every hackerspace will be able to produce MakAir” was not feasible, as it’s not the blueprints that are certified, but the industrial production process.
So the concept of distributed production, where each one produces three, wouldn’t work, as the machines themselves would not be standardised.
What was possible in hackerspaces was producing one Makair, working on it and eventually improving it. But afterwards, production would have to take place in an industrial space that’s identified and certified to the required ISO standards.
This realisation was a big disappointment for the team and many makers involved.
The maker's approach to using 3D printing allowed for rapid prototyping and saved thousands of hours. But they eventually turned towards something much more industrial since machining is faster, stronger and cheaper.
And on their way, they found other partners that would bring in the expertise and resources to certify their device:
At first, we set out like all the other makers in the world, we used Arduino boards, with defective servomotors, 3D printing, etc. The first versions were terrifying, but we had to advance somehow.
On the other side, we researched how we could industrialise and certify our ventilator, because a prototype is useless if you can’t mass produce it and have it certified so that doctors can use it.
It was during this quest that I ended up getting a call from Eric Huneker and his associate Marc Julien, directors of the medical company Diabeloop, who offered to help us with regulations.
The team was made up of Pierre-Antoine Gourraud in relation with the institutions, Diabeloop on regulations, my initial colleagues on documentation and engineering, and me for general management.
Within a week there were a hundred of us, all with well-defined roles. - Quentin Adam
Safety can be tricky when you allow decentralised manufacturing, especially in urgent and desperate situations, but ensuring that open source hardware is safe and reliable is essential.
Open devices like Makair or the Glia Project need to have their production sites approved by public institutions. However, that approval process takes time and resources, neither of which are readily available during a crisis like the COVID-19 pandemic.
That’s why it’s important that manufacturers, even those do-it-yourself hobbyists, do their due diligence and ensure their products are safe.
How? There are a few key steps recommended by André Rocha, coordinator of Fablab Benfica:
At the most basic level, test solutions with local health professionals
Be extremely careful during fabrication. Everything should be validated by professionals before use.
In projects that represent higher complexity, contact and involve public health authorities. They can help with the testing, and if it’s all good, help spread the solution on their website and ask other experts to contribute.
Step 4: Embrace existing institutions
Once Makair had clear technical specifications and a first group of contributors, they still needed money to go through expensive clinical trials.
So this is when they embraced traditional public institutions.
The teams led by Pierre-Antoine Gourraud and the university worked very conscientiously on submitting Makair’s project to a call for proposals from the French Army, and they were finally selected and raised 426.000 euros.
They also needed sophisticated tooling, like artificial lungs, to calibrate their machines. These artificial lungs cost 55,000 euros and were hard to find, so they called the distributors. But they knew the CEA, the French Alternative Energies and Atomic Energy Commission, had one.
They would eventually be invited to work directly at the CEA’s facilities, as it was simpler to send the team there, given the tests they needed to do.
Makair’s founders acknowledge that it was a mistake to call their collective Makers for Life.
One important thing that I want to tell the maker community: we called ourselves “Makers for Life”, but that was a mistake.
In fact, from the perspective of the industrial community, makers are more like Sunday hobbyists.
Makers need to realise that sometimes they have a divisive attitude about the industry, which offends people who should be allies. Fortunately, our project was perceived as coming from makers but having become industrial, given the makeup of the team. As is often the case in an industrial process, most of us didn’t know each other before, we were basically looking for engineers specialised in each aspect.
[…]
We were very quickly confronted with the problem of hooking up to the hospital’s oxygen network.
We chose not to follow this path, because after discussion with military doctors, we understood that in some cases they would end up intervening in gymnasiums that had been converted into hospitals in rural areas, where there would be no oxygen network.
- Quentin Adam
By involving experts in multiple fields, even institutions not used to collaborating with makers, the Makair collective was able to lift the successive obstacles slowing them down and come up with a much more robust, cheap and viable solution that wouldn’t have been possible with more traditional solutions.
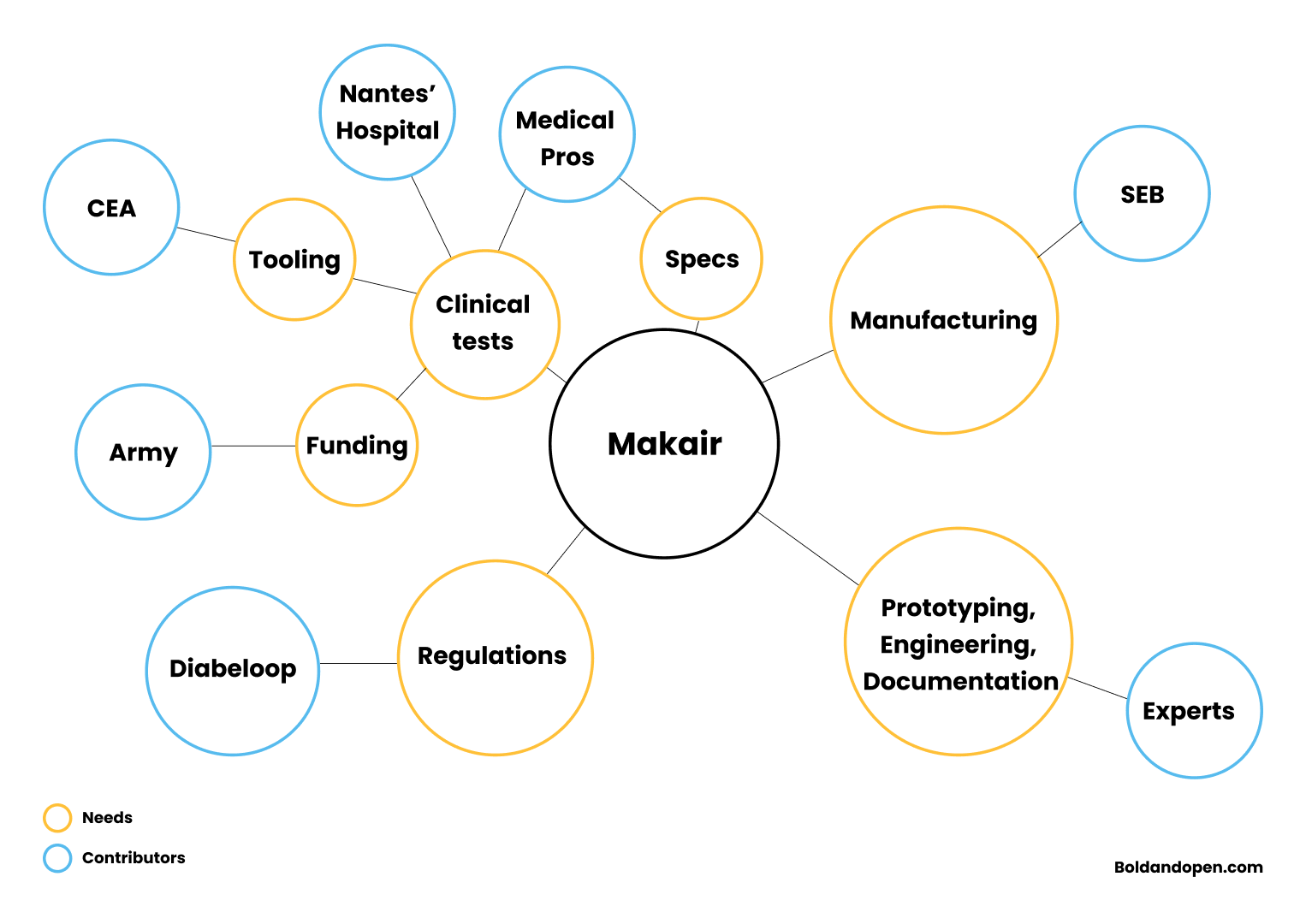
So as you understand the layers of problems you need to tackle, it can be useful to map your project’s needs and the actors who can contribute because they need the solution you’re trying to create, and they have the resources and skills you need.
For example, you can create a mindmap where you first map your needs (in mustard in the graphic below), and then you go through the potential contributors (in blue) who would be motivated to chime in:
Step 5: Be vulnerable about your shortcomings, and invite others (but not everyone) to fill in the gaps
By working in open source and publicly sharing your challenges, you motivate through collective innovation, because what’s created belongs to everyone and no one.
And on top of that, you enable those with the same problem or goal to connect with you and offer their contributions and advice.
But for people to know what to contribute, you need to communicate very clearly about what you’re missing or trying to achieve.
At the beginning, we didn’t really know what we were doing, but little by little we started to define our aeration system, consolidating each night. As we were working in open source, it wasn’t long before people started to contact us and offer advice. Our only response was: “We’re far from experts, can you help us?” So people got more and more involved, and that’s how we were able to integrate great expertise. - Quentin Adam
At the beginning, Makers for Life’s members tested seven ideas in parallel without worrying about being wrong, and finally arrived at a great result. They had managed to prototype a Makair that wouldn’t cost more than 1500 euros, against the tens of thousands of euros of other traditional respirators.
Often we expect open projects to be open to any contribution, but here time and quality were crucial, so they couldn’t deal with every possible contribution.
That’s why they created a filter for contributions to only accept the profiles they were missing:

Step 6: How to produce at scale
Making hardware at scale without compromising on quality or clinical security can be extremely time-consuming and expensive, unless you already have factories, experienced employees and processes in place.
At the beginning, the Auvergne-Rhône-Alpes region funded the manufacturing of the first prototypes, but later, the SEB group, an electrodomestic manufacturer, the drone maker Parrot, and the automaker Renault volunteered to fabricate several hundred units per day.

Going this fast would have been impossible if there had been patents to negotiate with these many parties.
The end result was that a few months after gathering a first community, this open source dynamic was able to kickstart the production of a few hundred devices that would cost around 1000 euros, ten to forty times less than a common respirator.
But making this device open source was not just about the cost, it was also about the innovation, since the fact that anyone could participate changed everything.
The Makair can now be deployed in new rural contexts where normal respirators are unaffordable, or customised by army engineers so they can understand and repair it, with the option of reconfiguring it remotely depending on the problem.
Doctors could use MakAir’s algorithm to manage air pressure, which they couldn’t do on closed machines.
This open approach has proven itself in software and other fields, but it is extremely powerful in times of crisis because it makes it easy for multiple actors to focus on the same problem at the same time and allows for a solution to spread worldwide and be adapted to every local context.
This open approach applies very well to all sorts of other engineering problems that already have a solution but are constrained by complex value chains and intellectual property barriers.
It also applies well to products that suffer supply gaps, which is the case in most innovations where the majority of the world’s population has little or no access to them.
At the beginning, hospital personnel were pretty sceptical. Doctors didn’t really believe that a bunch of geeks who knew nothing about the medical environment would be able to create from scratch an operational respirator in four weeks and share the blueprints in open source without trying to profit from it.
But when they saw the first prototypes working, everyone was cheerful to see the first test results with patient simulators.
Makair’s journey contains lessons we can reuse in a world in transition with more questions than answers. If we take the opportunity to lead and connect people together, we can unlock powerful ways to create ambitious and robust solutions when crises strike, even when we don’t know what we need or lack many crucial skills and resources.
TL;DR
Understanding the problem you face.
As the Covid pandemic broke, Makair’s founders sought to understand the issues with Covid and prioritise the one’s that they could respond to. In this case, they decided to focus on the respirator shortage.To form an Ecosystem, set up an ambitious mission to create a key piece of the crisis solution, but start small.
Invite the first essential people you need solve part of the problem and lend you some credibility. Ideally, these are the people who will help you define the specification a solution needs to meet, which you can later share with the next contributors and start building.To create better solutions, don’t copy what already exists. Start from first principles.
Makair didn’t have any medical experience, and they needed to create a respirator that was cheap, made with tools and parts easily available globally and easy to manufacture at scale. So they could not copy what was already on the market. By breaking down the problem into its most fundamental elements, they could come up with the simplest components they needed to build their ventilator.Map the ecosystem you need to mobilise
As new obstacles arise, map the problems you can’t tackle on your own. Then map the actors who can contribute the resources and skills you need and would be motivated to help because they need the solution you’re trying to create.Be vulnerable and open about your shortcoming. This enables others (but not everyone) to fill in your gaps.
The Makair project had no medical expertise, no manufacturing capacity, no tooling or funding, and no experience certifying medical equipment, but by sharing their needs, they were able to invite or attract experts from public and private institutions who would bring in their missing skills and resources.
Sources
What can we learn from the makers who organized to locally produce open source respirators?, by Bérengère Fally
OPEN-SOURCE MEDICAL HARDWARE: WHAT YOU SHOULD KNOW AND WHAT YOU CAN DO, by Victoria Heath
MakAir, an open source ventilator in the making, by Ewen Chardronnet
L'aventure du MakAir, by Innovation Citoyenne and Le Monde
Entre Nantes et Grenoble, une course contre la montre pour créer un respirateur artificiel à bas coût, by Yan Gauchard